Results & Facial Changes
Do Braces Change Your Face Shape? The Real Before & After (2026 Guide)
Quick Answer
Braces move teeth, not facial bones — but tooth position controls how your lips and cheeks are supported, so your face can look noticeably different after treatment. The most visible changes happen at the lips (front teeth pushed backward reduce lip fullness; teeth moved forward increase it), the smile width (arch expansion creates a broader smile), and the side profile (extraction cases where premolars are removed often flatten the lower face slightly). Bone structure does not change from braces alone. For patients still growing, changes can be more significant because the jaw is still developing.
Part of the Results & Facial Changes Guide — how braces reshape your face, jawline, lips, and profile.
What Braces Actually Move (And What They Don't)
Braces apply continuous, controlled force to teeth via archwires and brackets. That force moves teeth through the alveolar bone — the portion of the jaw that holds the tooth roots. Bone remodels around each moving root: it dissolves on the pressure side and deposits new bone on the tension side, allowing teeth to travel millimeters over months.
What braces do not move: the basal bone (the main body of the mandible and maxilla), the nasal bones, the zygomatic arches (cheekbones), or any other facial skeleton. Orthodontics is a soft tissue story told through tooth position.
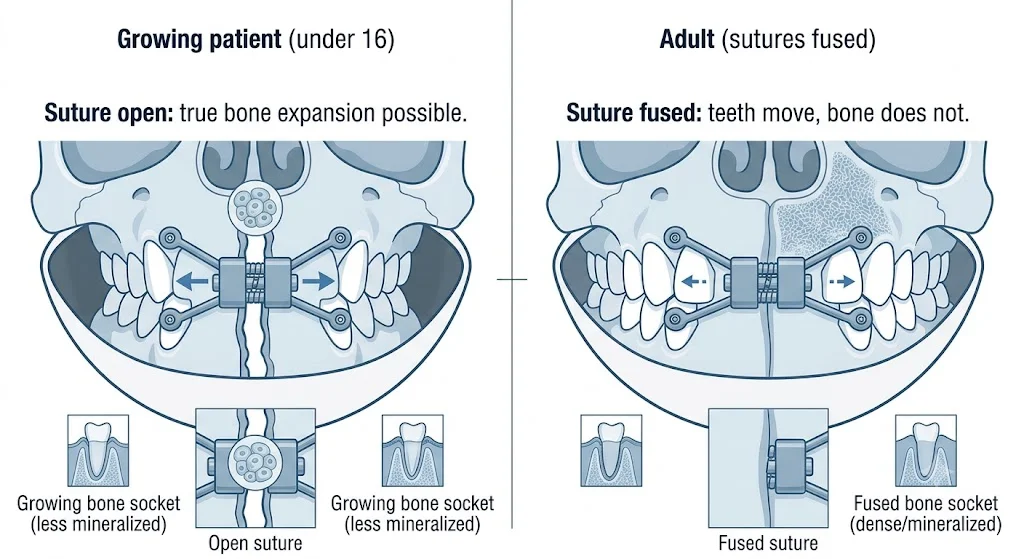
The one exception: palate expanders in growing patients. A rapid palate expander (RPE) splits the mid-palatal suture — a growth plate in the roof of the mouth — and widens the upper jaw itself. This is true bone change, not just tooth movement. It works in patients under approximately 15 to 16 years old, before the suture fuses. Adults who need palate expansion require surgery (surgically-assisted rapid palate expansion, or SARPE).
The Lip Change: Why It's the Most Visible Result
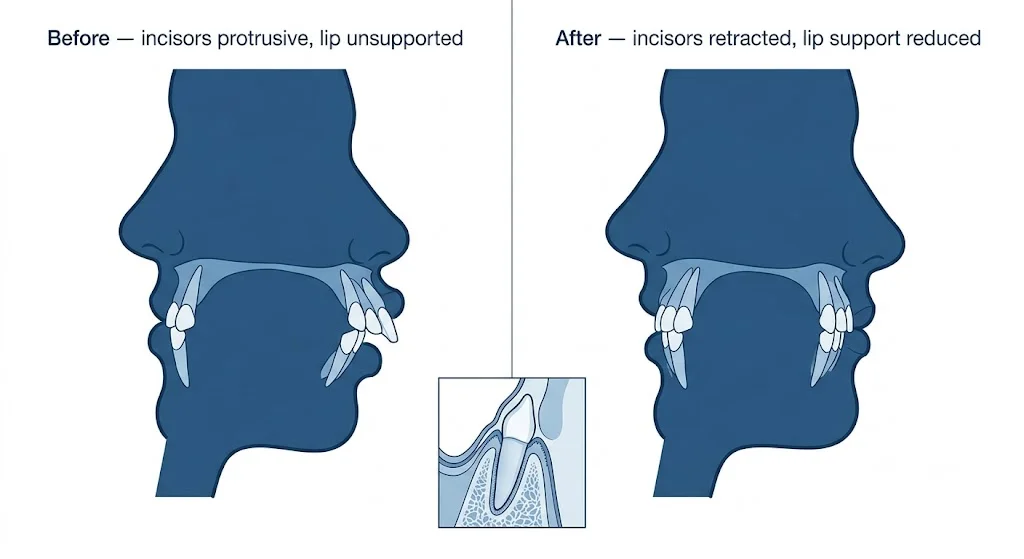
Your upper and lower lips rest against your front teeth. The angulation of those teeth — how far forward or backward they tip — determines how much support the lips get from behind.
This is why orthodontists measure lip-to-incisor relationship in their treatment planning. The angle of the upper central incisors to a reference line (typically the Frankfort horizontal or the SN plane) is one of the most tracked measurements in an orthodontic case.
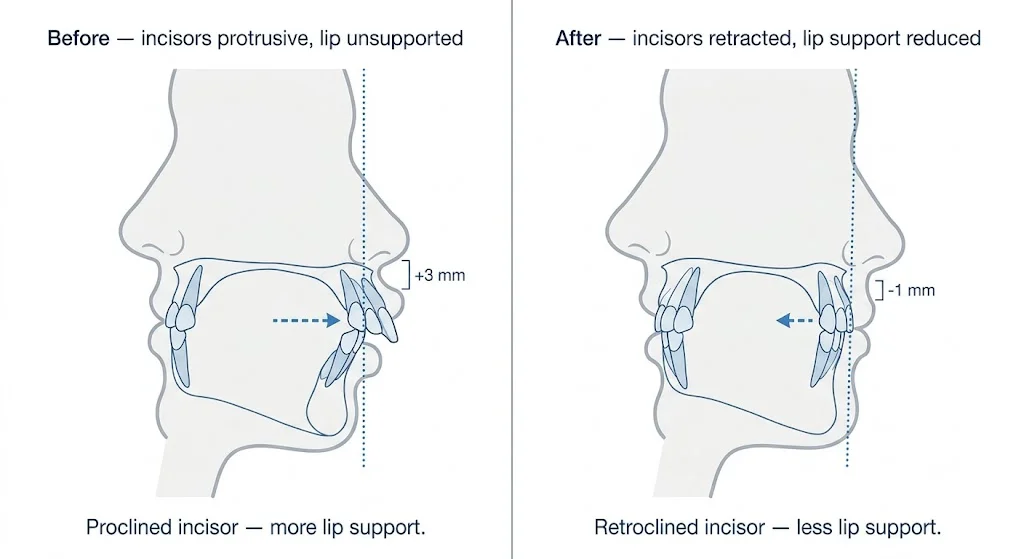
- When front teeth move backward (retraction): lip support decreases, the upper lip becomes slightly flatter, and the distance from the upper lip to the Ricketts E-plane (a reference line from nose tip to chin tip) increases. In profile, the lip looks less prominent.
- When front teeth move forward (proclination): lip support increases, the upper lip appears fuller, the profile softens. Common in cases treating deep overbites or very upright incisors.
Neither direction is universally better. Orthodontists aim for lips that fall within established soft tissue norms for a balanced profile, which varies by ethnicity and individual facial structure.
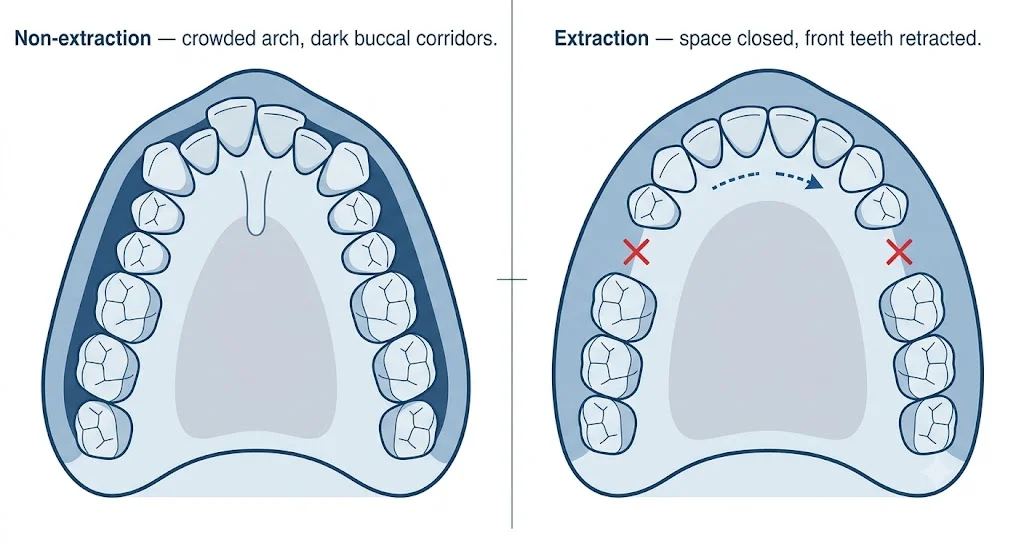
Extraction vs. Non-Extraction: Two Very Different Outcomes
The most significant predictor of how much your face changes from braces is whether teeth are extracted.
Extraction Cases (Premolar Removal)
When a patient has severe crowding or bimaxillary protrusion (where both upper and lower front teeth are excessively forward), the orthodontist typically removes the first premolars on each side — creating four gaps — and uses that space to retract the front teeth backward. This reduces lip protrusion significantly, flattens the lower third of the face, and creates a straighter profile.
The change in lip position in extraction cases is measurable and permanent. Studies using cephalometric analysis consistently show 1 to 3 mm of upper lip retraction for every 4 to 5 mm of incisor retraction, with a roughly 60 to 70% soft tissue response ratio to tooth movement.
Non-Extraction Cases
Most cases today are treated without extractions, using arch expansion, interproximal reduction (IPR — minor enamel reshaping between teeth), or simply alignment within the existing arch space. In these cases, lip position changes minimally, smile width often increases as teeth spread laterally, and the overall profile stays largely the same. The change is more about smile aesthetics than overall face shape.
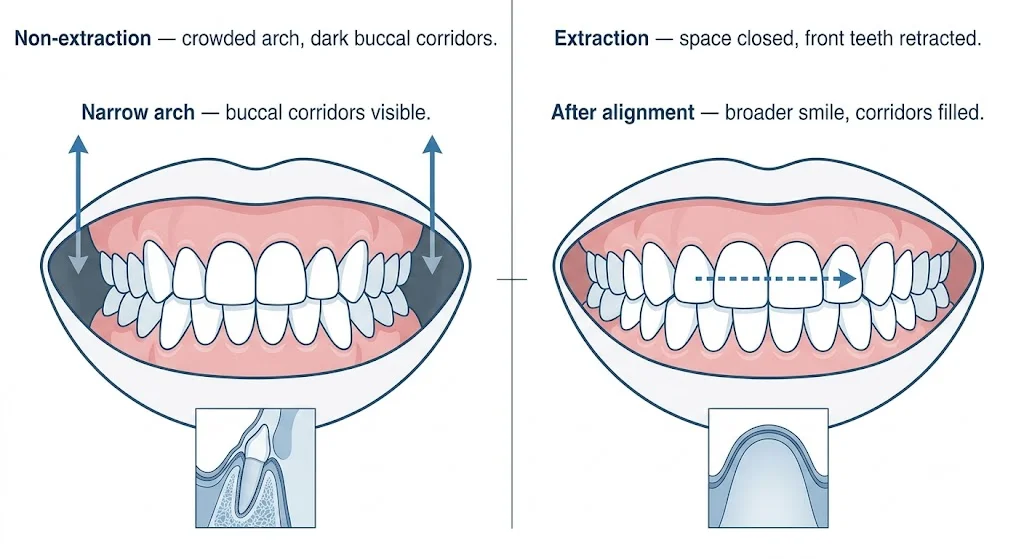
Smile Width: The Change You See Head-On
Looking straight ahead, the most visible change from braces is usually smile width — how many teeth show when you smile broadly.
A narrow arch (common in patients with crowding) means posterior teeth collapse inward, leaving dark buccal corridors — shadows at the corners of the smile. Arch expansion or simple alignment can widen the dental arch, filling those corridors with tooth structure and creating a broader, more uniform smile. This is not a bone change — it is teeth aligning along a wider arc of the same jaw — but the visual result is one of the most commonly cited improvements patients notice after braces.
Growing Patients vs. Adults: Why Age Matters
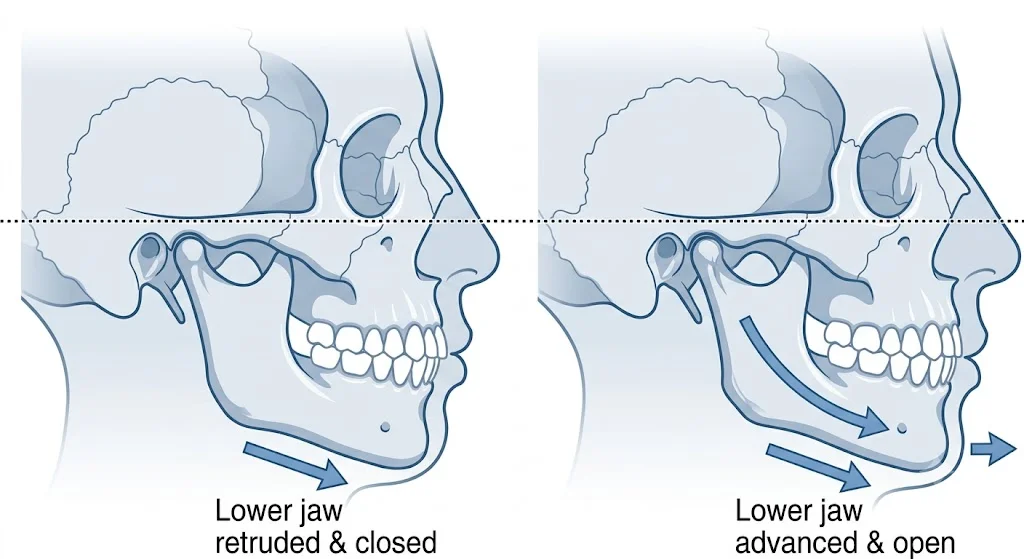
In patients who are still growing — generally under 16 for girls and under 18 for boys — orthodontic treatment can interact with natural jaw development. Functional appliances (Herbst, Twin Block, headgear) used during growth can influence how the upper and lower jaws develop relative to each other. This is true skeletal change, not just tooth movement.
For adults, the jaw has finished growing and the sutures are fused. Braces can only move teeth within the existing bone envelope. The soft tissue changes are real and visible, but the underlying skeleton stays where it is. This is why orthodontists who treat children can achieve results — particularly in correcting jaw size discrepancies — that are simply not possible in adults without surgery. An adult with a significant underbite or severe skeletal Class II (receded lower jaw) needs orthognathic surgery to move the jaw; braces alone can only camouflage the discrepancy by tilting teeth to compensate.
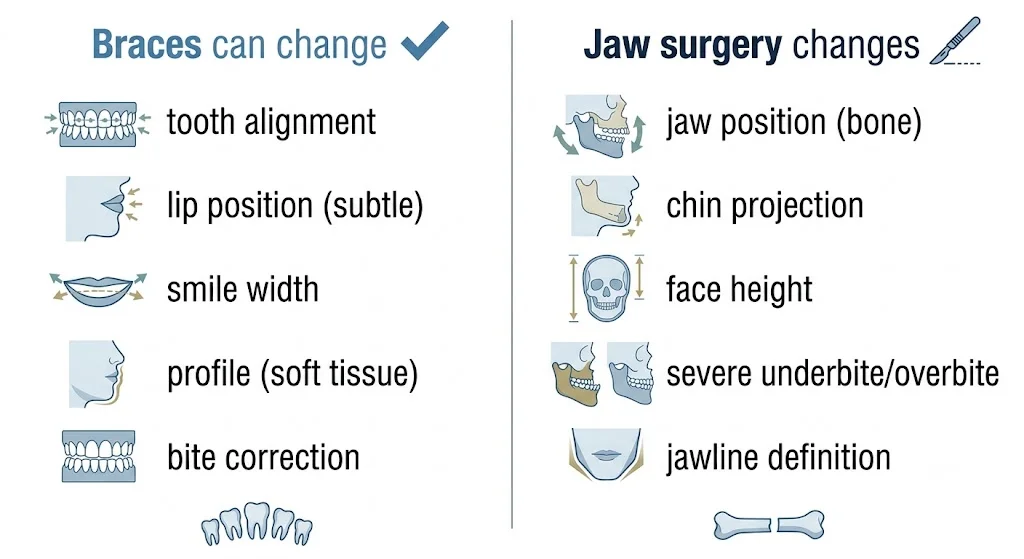
What Braces Cannot Change (That's Jaw Surgery Territory)
Patients who want dramatic facial restructuring need to understand the line between orthodontic and surgical treatment. Orthognathic surgery moves the jaw bones themselves — the Le Fort I osteotomy moves the upper jaw forward, backward, up, or down; the BSSO (bilateral sagittal split osteotomy) moves the lower jaw; genioplasty repositions the chin bone. These procedures produce skeletal changes that braces cannot replicate.
Patients who see dramatic transformations online often had combined orthodontic and surgical treatment — not braces alone. Braces alone cannot move the chin forward or backward, shorten or lengthen the face vertically, change the shape of the nose, reposition the cheekbones, or correct a severe underbite or overbite rooted in jaw size discrepancy.
Realistic Expectations: What You'll Actually See
Most patients with standard orthodontic cases see smile alignment and symmetry (always — this is the primary goal), subtle lip changes (usually 1 to 2 mm of movement in extraction cases, minimal in non-extraction cases), slight profile improvement (especially if pre-treatment teeth were very protrusive), and a wider smile in crowding cases with arch development.
The transformation photos that go viral on social media often involve teenagers whose faces also changed due to natural growth during the treatment period, before photos taken with bad lighting or closed-mouth expressions, weight loss during a 2-year treatment period, or surgical cases labelled as braces alone.
Your orthodontist can show you cephalometric projections — predicted soft tissue changes based on the planned tooth movements — before treatment begins. This is the most accurate way to know what your specific case will produce.
Curious about the full timeline?
Face changes unfold month by month as teeth move. Read our complete timeline guide to understand exactly what happens at each stage of treatment.
Read the Timeline Guide →